
Does Osteopathic Manipulation Lead to Improvements in Physical and Muscle Mechanical Function and Spinal Symmetries in Golfers?
¿La Manipulación Osteopática Mejora la Función Mecánica y Física y la Simetría Espinal en Golfistas?
Daniel Rojas-Valverde1, Alejandra Sánchez-García2, David Sáez-Ulloa1 y Randall Gutiérrez-Vargas1
1Centro de investigación y diagnóstico de la salud y Deporte. Escuela Ciencias del Movimiento Humano y Calidad de Vida. Universidad Nacional, Heredia, Costa Rica
2Comité Olímpico de Costa Rica, San José, Costa Rica.
Artículo publicado en el journal Kronos, Volumen 18, Número 1 del año 2019.
Publicado 20 de junio de 2019
Resumen
Palabras clave: terapia alternativa, osteopatía, aptitud física, golf
Abstract
Keywords: alternative therapy, osteopathy, physical aptitude, golf
INTRODUCTION
Golf in Costa Rica has become in a highly-rated, popular professional and amateur sport. Due to the sport characteristics, injuries can become a very common issue among golfers. In sports like golf, different conditions such as changes in muscle stiffness and imbalance (which cause movement dysfunction) can lead to pain or discomfort during a competition. As muscles tighten, they sometimes get weaker, reducing the efficiency of body flow during movement (Cabri, Souse, Kots, & Barreiros, 2009; Kim & Sung, 2009).
Brandon and Pearce (2009) reported that significant stress on shoulders, elbows, wrists, and lower back affects the swing biomechanics. These areas coincide with the most common injured structures in golfers due to the sport’s singular technique. The movement disturbance is usual among golfers because of the repetitive movements and high- velocity actions that occur during swing, and may lead to injuries (Burdorf, Van der Steenhoven & Tromp-Klaren, 1996; McHardy & Pollard, 2005).
Asymmetries and high muscle stiffness can decrease physical characteristics such as strength or sport performance (Bae, Kim, Seo, Kang & Hwang, 2012, Kim & Sung, 2009; Rojas-Valverde et al., 2018), hip and lumbar muscle coordination (Lindsay & Horton, 2010), hip and lumbar rotation and extension (Vad, Bhat & Basrai, 2004) among others.
The medical community has intervened in several different ways to prevent injuries caused by these repetitive movements in sports. For that reason, physical therapy and prevention assessment techniques are required (Sánchez-Ureña, Rojas-Valverde & Gutiérrez-Vargas, 2018). Osteopathic physicians specialize in body mobilization, not only the spine but also soft tissues, muscles, nerve flow, blood flow, lymph flow, myofascial release, as well as techniques such as cranial-sacral (Alderman, 2009). Successful treatment could restore the range of movement, improve symmetry, reduce muscle hypertonicity and restore normal joint receptor activity (Williams, 1997). Likewise, osteopathic manipulation has been considered a methodology for the management of spinal pain, a condition commonly suffered by golfers (Snow, 2016). Osteopathic manipulation as a way of treatment can be successful to restore spine symmetry and enhance sport performance factors among golfers (Cole & Grimshaw, 2015; Lejkowski & Poulsen, 2013).
However, the impact in mechanical and physical performance is not well known. For this reason, the purpose of our study will be to analyze the effectiveness of global osteopathic manipulation on the improvement of the mechanical and physical function and spine imbalance reduction in golf players.
METHODS
Subjects
10 male Costa Rican nationally ranked golfers (age 32.9 ± 13.2 years, weight 80.8 ± 19.4 kg, height 1.8 ± 0.1 m) were part of this study. They had an average of 3.8 ± 1.7 golf training sessions/week and had an average of 9.9 ± 1.4 years of golf experience. All participants were right handed. As inclusion criteria it was set that all participant were active golf player of the top division of Costa Rican League, were all 18 or more years, were ranked in the top 10 best players in local League and had no neuromuscular disorders or injuries in the last 6 months.
Ethical statement
All subjects were informed of the details of the experimental procedures, as well as the associated risks and discomforts. Each subject signed a written informed consent contract according to the criteria of the Declaration of Helsinki regarding biomedical research involving human subjects (64th WMA General Assembly, Fortaleza, Brazil, 2013). All procedures were approved by the School of Human Movement and Quality of Life Academic Council (Linked to SIA-0025-16) and Sport Training Program of the Costa Rican Olympic Committee.
Experimental Protocol
This study followed a transversal and semi experimental design with one group and two assessments (pre-post). A 30 min osteopathic manipulation (OM) was made between measures. There was a pre-post OM assessment in Trunk Rotational Mobility Test (TRMT), Back Skin Temperature (Back Skin T°), Time of Contraction (Tc) and Maximal Voluntary Isometric Strength (MVIS) (see figure 1 and figure 2).
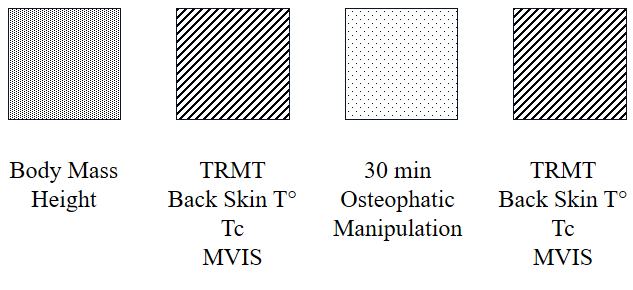
Figure 1. Study design.
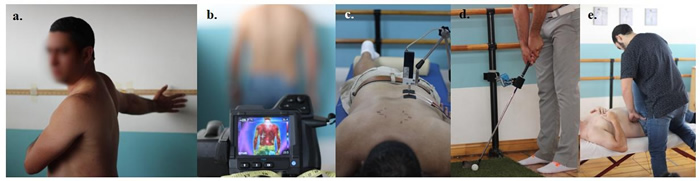
Figure 2. Assessments and intervention images. (a) Trunk Rotational Mobility Test (b) Back Skin temperature. (c). Time of Contraction. (d). Maximal Voluntary Isometric Strength. (e). e.g. Osteopathic Manipulation Techniques.
Instruments and Procedures
Body composition
To evaluate body composition an HD-313 Tanita (Tanita Corporation®, Tokyo, Japan) was used to assess the total body mass (kg) with a precision of ± .1kg. Height was measured using a wall stadiometer.
Trunk Rotational Mobility Test
Participants were asked to perform a two-sided (Right (R) and left (L)) trunk rotation and reach a specific mark in the wall. Subjects had to stand 60cm far from the wall, keep feet at shoulder width (40cm) and no hip compensation was allowed (Perry et al., 2004). Two maximal rotation reaches were conducted and the highest rotation was recorded for each side. The coefficient of variation for each side was 0.11% (R) and 0.09% (L). Test-retest reliability showed a ICC of .869 (.56; .97) (R) and .711 (.19; .92) (L) in pre-post measurement, and previous reliability data reported in inter-evaluator assessments (.9; Perry et al., 2004).
Skin Temperature
Skin temperature was assessed using an Infrared Thermography Camera (IRT) (FLIR T4 Series), set 2 meters from the participant’s back. Emissivity was set to 0.98. Subjects were instructed to stand for 10 min at room temperature with their feet at shoulder width (40cm). Back hemi lateral photos was taken, mean temperature of two areas were analyzed from each side, area 1, from C7-T5 and area 2, T5-L5. This kind of assessment has been used in sport applications previously to see how activation could influence skin temperature (Gutiérrez-Vargas et al, 2017).
Muscle Time of Contraction and Lateral Symmetry Index
Tensiomyography was used to assess muscle time of contraction (Tc, ms), delay time (Td, ms) and muscle displacement (Dm, mm) in trapezius middle (TM) and erector spinae (ES), from both sides (R and L). These muscles were selected because of their fundamental role in specific golfing kinematics, control and stabilization and their injury incidence in this sport (Bae, Seo, Kang & Hwang, 2012).
For TM and ES measures, the participants laid relaxed in prone position and a cushioned pad was used to fix the knee joint at 150º. After sterilizing the area, two 5 cm2 adhesive electrodes (TheraTrode®, TheraSigma, California, United States of America) with an inter-electrode distance of 5-cm were placed in the respective muscles, avoiding tendons insertions (García-García, Cancela-Carral, Martínez-Trigo & Serrano-Gómez, 2013; Rojas-Valverde et al., 2016). The measurement point was set at the maximal muscle belly of each muscle, which was established visually. Palpation of the muscles during a voluntary contraction were also measured (De Paula-Simola et al., 2015; Rojas-Valverde et al., 2015). The electrodes were connected to an electrical stimulator (TMG-S2 d.o.o., Ljubljana, Slovenia), that triggers a quadrangular, monophasic, 1 ms pulse duration. A digital displacement transducer (GK 40, Panoptik doo, Ljubljana, Slovenia) was positioned perpendicular to the previously established measurement points of the muscle belly with an initial constant spring (De Paula-Simola et al., 2015). The measurement instrument started triggering a 40mA electrical stimulus to induce muscle contraction. The electrical stimulus was increased by 20mA until the maximal Dm was obtained (~100mA) (Sánchez-Ureña, Rojas-Valverde & Gutiérrez-Vargas, 2018). The electrical stimuli were induced in lapses separated by 10 s to avoid fatigue or post-tetanic activation (De Paula-Simola et al., 2015, 2016). From the TMG measurements, the following parameters were obtained: all TMG variables used have demonstrated a high intraclass correlation coefficient (0.86-0.98) in previous studies (De Paula-Simola et al., 2015, 2016).
Lateral symmetry index (LSI) variables were assessed by the following formula (Rojas-Valverde et al., 2018):

According to Bishop, Turner and Read (2018), when symmetry is lower than 90%, asymmetry should be considered.
Maximal Voluntary Isometric Strength
The maximal isometric strength was measured by asking the subject to exert the highest isometric strength in the impact phase of the golf swing in both sides (R and L). A digital dynamometer was used (OCS-L, KlauTM, Japan), with a capacity of 2-300kg, and a resolution of 0.1kg, accuracy class OIML III. An iron (Callaway X24) was gripped from the end of the grip to a stable structure 40cm height from the floor. Two maximal isometric actions were measured and the highest was recorded for each side. The coefficient of variation for each side was 0.07% (R) and 0.07% (L). Test-retest reliability showed a ICC of .701 (.16; .84) (R) and .742 (.25; .93) (L) in pre-post measurement.
Osteopathic Assessment
The treatment protocol was based on an initial evaluation conducted in prone position that included the following tests: Sclerotome Palpation Test, Mitchell´s Lumbar Test and Sclerotome`s Test on Articular Apophysis. The following tests were performed in supine decubitus position: Tomas Test and Mitchell Test for the cervical spine. Moreover, these tests were conducted with the patient in a sitting position: Test of the Ascending Thumbs in Sitting Position according to Mitchell, Mitchell Test for High Dorsal Vertebrae, Piedallu Test. With the patient standing, the following tests were used: Gillet test, Lumbar Analytical Mobility Test. The tests described are commonly used by osteopaths (Beal, 1989; Espinosa-Carrasco, 2008; Martínez, 2002).
After identifying the movement dysfunctions, the specialist proceeded to administer the protocolary treatment, which includes high-speed osteopathic techniques (thrust techniques), muscle energy techniques, positional release techniques and myofascial techniques.
The techniques were performed in a cephalic-caudal order, starting with the high-speed osteopathic techniques: Fryette's OAA, Thumb move lying face down for C7-T1, Dog Technique for middle thoracic vertebrae, Fryette Technique for low thoracic vertebrae, Thrust Technique for sacral torsion dysfunctions, Global Technique of the pelvis (Shearar, Colloca, White, 2005). Furthermore, soft tissue techniques were performed in the following order: Muscle Energy Technique for the scalene, Neuromuscular Technique of bilateral psoas muscle, Bilateral Pyramidal muscle stretch, Flexion Stretch Technique for interspinous ligaments, Stretching Technique for bilateral iliolumbar ligaments. Finally, a Lumbar Myofascial Technique was used. All these techniques are commonly used by osteopaths in their daily attention (Fryer, Morse & Johnson, 2009; Johnson & Kurtz, 2003).
Statistical Analysis
Descriptive statistics were implemented through the mean (M) and the maximum and minimum measures. The normality of the data of each of the variables was checked via the Shapiro-Wilk Test and the Levene Test for Homogeneity of Variance. Data of TRMT, Skin Temperature, TMG, MVIS and LSI were analyzed by using repeated measures of the t-test (pre and post-manipulation) and with an alpha set at p< 0.05. The magnitudes of the differences were analyzed using d-Cohen for t-test analysis categorized as follow: d= 0.2 as small, d= 0.5 as moderate, and d= 0.8 as large effect size (Cohen, 1988). Changes were presented in percentage of change (Δ%). An alpha was set prior at p< .05. Test-retest reliability (intra class correlation coefficient, ICC) was performed in all assessments using the intra class correlation coefficient (ICC). Data analysis was performed using the Statistical Package for the Social Sciences (SPSS, IBM, SPSS Statistics, V 22.0 Chicago, IL, USA).
RESULTS
Results suggested statistical differences between measures in TRMT (d= 0.53-1.67, moderate-large), dorsal and lumbar skin temperature (d= 0.02-0.24; small). Mechanical function presented differences in TM and ES muscle in TMG variables as Tc, Dm and Td (d= 0.09-0.26; small), and MVIS (d= 0.24-0.33, small) (see table 1.).
Table 1. Pre-post osteopathic manipulation comparison of physical and muscle mechanical variables.
There were found differences in lateral symmetry of TRMT (d= 0.55, moderate), Dorsal and lumbar temperature (d= 0.16-0.27, small), TM and ES muscles in Tc (d= 0.02-0.14, small) and MVIS (d= 0.5, moderate) (see table 2.). Asymmetry was assumed in pre-post LSI in: TRMT, TM and ES-Tc and MVIS.
Table 2. Pre-Post Lateral Symmetry Index comparison of physical and muscle mechanical variables.
DISCUSSION
Trunk Rotational Mobility
A 30 min osteopathic manipulation (OM) session managed to cause a moderate increase in contralateral mobility (which was achieved through various techniques), a slight improvement of the mobile imbalance between the dominant and non-dominant hemisphere. This is due to the ability of osteopathic techniques, some of which are of myofascial release and stretching, to improve the mobility of the segments. Lewit (1991) states that the increase in mobility of trunk rotation had mechanical changes triggered by the manipulation of the middle and lower lumbar segment, leading to positive effects in these areas such as the decrease of mechanical stress exerted on the soft and hard paraspinal tissues. An important consequence of these mechanical changes triggered by osteopathic manipulation, which is formulated as a hypothesis, could be the restoration of the mobility of the interapophyseal articulation and joint set. Triano (2001), indicates that a vertebral manipulation causes a re-establishment of muscular contractile capacity, enabling the patient to perform pain-free movements. Specifically, in mechanical properties, myofascial release and muscle stretching, two common OM techniques, have been shown to be effective in improving mechanical function (García-Manso et al., 2015).
Back Skin Temperature
Muscle activation by osteopathic techniques could have caused an increase in muscular and integumentary activity in the present study is shown a small different between pre and post OM assessments. The therapist's manual and mechanical contact with the skin of the patient causes an increase in skin temperature, and muscular energy techniques, among other osteopathic methods, can cause an acute metabolic increase in the area. The combination of these methods will facilitate the kinetic theory causing the necessary heat effect to decrease the restitution power of connective and dense tissues (Towlson, Midgley & Lovell, 2013).
The stretching techniques performed as part of the osteopathic therapy during the study, and the tensions produced consequently, result in muscular activation, whose main benefit is to increase the temperature of the muscle as well as its bloodstream to improve the delivery of the metabolic fuel to the active muscle (Rodríguez-García & Moreno-Murcia, 1997).
Muscle time of Contraction and Maximal Voluntary Isometric Strength
Small differences in muscle time of contraction and maximal voluntary isometric strength were found after OM. Osteopathic manipulation of muscle energy can lead to Sherrington’s muscle activation and reciprocal inhibition (Campos, 1998), that can cause an increase in the speed at which the muscle contracts and the amount of muscles recruited for this contraction due to isometric stimulation. This is caused by the constant stretching and muscle activation processes when performing these osteopathic techniques. According to studies that employ spinal manipulation, it is evidenced that the effects of spinal manipulation on paraspinal EMG activity can be associated with increases in muscle strength (Suter, McMorland, Herzog & Bray, 2000). Similarly, Keller & Colloca (2000) found that erectile vertebral isometric force, evaluated with EMG activity, increased after a spinal manipulation session compared with other manipulation techniques. More evidence suggest that manipulation as proprioceptive techniques and myofascial release has effect on strength performances (Robles, 2010; Rubini, Pereira & Gomes, 2005). The large and small increase in mechanical function and strength respectively, in the present study may be caused due to a greater number of actin-myosin bridges caused by osteopathic techniques, for example muscle energy techniques.
Imbalance Improvement
One of the objectives of osteopathic therapy is the achievement of optimal postures that allow fluid and coordinated movements at the muscular level. The muscle imbalances that affect golfers are those caused by the inhibition of phasic muscles and the increased activity of tonic muscles due to the constant employment of these muscles during sports. The small improvement of mechanical and functional imbalance evidenced in the study is possible because practical osteopathy served to normalize the entire muscle chain by restoring the mobility of the contractile and structural elements. This normalization was triggered by the inhibition of alpha and gamma neuromotors, intra and extrafusal, which according to Campos (1998), is caused by the manipulation with thrust techniques. Furthermore, thanks to Sherrington's reciprocal inhibition caused by the muscular energy techniques performed, a stabilization in muscle activity occurs by reducing the muscular stiffness of tonic muscles caused by physical activity.
Although there are small to moderate changes in the temperature of the symmetry improvement, skin temperature, muscle contraction´s time and isometric strength, these results do not show significant differences. Therefore, these results must be analyzed with caution. There were significant changes in trunk rotational mobility but in most of the variables were no differences and in some cases a decrease in physical function was found. These results could compromise the physical performance of golfers during competition, these could lead to new strategies regarding when and how does the OM have to be apllied.
Considering the sample size and the level of training, these results have to be confirmed in further studies, including other fundamental variables in the understanding of the movement of this sport. As another limitation, there were moderate to high reliability results of the testes in TRMT but the confidence intervals was poor to very good. Due to the lack of access to data, other TMG variables as sustain time and muscle time to relation were no considered for analysis, these other variables could bring a wider approach of the effectiveness of OM in golfers.
Coaches and athletes should consider that the changes shown in the present investigation may affect athletic performance, so it should be evaluated when and how this type of intervention should be performed. Some manipulation techniques could lead to physical and physiological changes that could lead to decrease in performance, this new evidence should be addressed by osteopaths and physical therapist in order to develop new intervention strategies in sports.
PRACTICAL APPLICATION
A 30min-general osteopathic manipulation session tends to lead to a moderate to large increase in trunk mobility, and small but no significant changes in dorsal and lumbar skin temperature, increased strength and a shorter time of muscle contraction. This osteopathic intervention tends to upturn spinal contralateral imbalance in flexibility, dorsal skin temperature and muscle contraction time of erector spinae, but these changes were not significant, in fact, there were a decrease in physical function in some of the variables as: skin temperature, time of contraction, Maximal Voluntary Isometric Strength. More studies are required to pursue the osteopathic manipulation in golf technique and performance, and it beneficial or prejudicial effect on time.
Referencias
1. Alderman, D. (2009). Why Prolotherapy is the Strongest Weapon I have found against Chronic Pain and Sports Injuries. Journal of Prolotherapy, 1(2)., 104-106.
2. Bae JH, Kim DK, Seo KM, Kang SH, Hwang J. (2012). Asymmetry of the Isokinetic Trunk Rotation Strength of Korean Male Professional Golf Players. Annals of Rehabilitation Medicine, 36(6)., 821-827. https:// doi.org/10.5535/arm.2012.36.6.821
3. Beal, M. (1989). The principles of palpatory diagnosis and manipulative technique. OH, USA: American academy of Osteopathy.
4. Bishop, C, Turner, A., Read, P. (2018). Effect of inter-limb asymmetries on physical and sport performance: a systematic review. Journal of Sport Science, 36(10)., 1135-1144.
5. Brandon, B & Pearce, P.Z. (2009). Training to prevent golf injury. Current Sport Medicine Reports, 8(3)., 142-146. doi: 10.1249/JSR.0b013e3181a61c88
6. Burdorf, A., Van Der Steenhoven, G.A., Tromp-Klaren, E.G. (1996). A one-year prospective study on back pain among novice golfers. American Journal of Sports Medicine, 24, 659-64.
7. Campos, G. (1998). Terapia manual y osteopatia. De la teoria a la técnica. Revista Iberoamericana de Fisioterapia y Kinesiología, 1(1)., 47-59.
8. Cabri, J., Sousa, J.P., Kots, M. & Barreiros, J. (2009). Golf-related injuries: a systematic review. European Journal of sport Science, 9(6). https:// doi.org/10.1080/17461390903009141
9. Cohen J. (1988). Statistical power analysis for the behavioural sciences. Hilsdale. NJ: Lawrence Earlbaum Associates.
10. Cole, M. H., & Grimshaw, P. N. (2015). The Biomechanics of the Modern Golf Swing: Implications for Lower Back Injuries. Sports Medicine, 1-13.
11. de Paula Simola, RA, Harms, N, Raeder, C, Kellmann, M, Meyer, T, Pfeiffer M, and Ferrauti, A. (2015). Assessment of neuromuscular function after different strength training protocols using tensiomyography. J Strength Cond Res, 29, 1339-48.
12. de Paula Simola, RA, Raeder, C, Wiewelhove, T, Kellmann, M, Meyer, T, Pfeiffer, M, and Ferrauti, A. (2016). Muscle mechanical properties of strength and endurance athletes and changes after one week of intensive training. J Electromyogr Kinesiol, 30, 73-80.
13. Espinosa-Carrasco, J. (2008). Efectividad del tratamiento osteopático en pacientes con latigazo cervical. Revista fisioterapia, 7(1)., 03-12.
14. Fryer, G, Morse, CM, Johnson, JC. (2009). Spinal and sacroiliac assessment and treatment techniques used by osteopathic physicians in the United States. Osteopath Med Prim Care, 14, 3-4.
15. García-García, O., Cancela-Carral, J. M., Martínez-Trigo, R., and Serrano-Gómez, V. (2013). Differences in the contractile properties of the knee extensor and flexor muscles in professional road cyclists during the season. J. Strength Cond. Res., 27, 2760–2767. doi: 10.1519/JSC.0b013e31828155cd
16. Gutiérrez-Vargas, R., Ugalde-Ramírez, A., Rojas-Valverde, D., Salas-Cabrera, J., Rodríguez-Montero, A. & Gutiérrez-Vargas, J.C. (2017). La termografía infrarroja: ¿Herramienta efectiva para diagnosticar áreas musculares fatigadas después de correr un maratón? Revista Facultad de Medicina, 65(4). , 601-607.
17. Johnson, SM. & Kurtz ME. (2003). Osteopathic manipulative treatment techniques preffered by contemporary osteopathic physicians. J Am Osteopath Assoc, 103(5)., 219-24.
18. Kim, H. & Sung, K. (2009). The influence of long term golf participation on spinal asymmetries, power of lower extremities, and EMG activities of rotator muscle. Exercise Science, 18(4)., 517- 526.
19. Keller, TS., Colloca, CJ. (2000). Mechanical force spinal manipulation in- creases trunk muscle strength assessed by electromyography: a comparative clinical trial. J Manipulative Physiol Ther, 23, 585-95.
20. Lejkowski, P. M., & Poulsen, E. (2013). Elimination of intermittent chronic low back pain in a recreational golfer following the improvement of hip range of motion impairments. Journal of Bodywork and Movement Therapies, 17(4)., 448-452.
21. Lewit K. (1991). Manipulative therapy in rehabilitation of the locomotor system. Oxford: Butterworth-Heinemann.
22. Lindsay, D. & Horton, J. (2010). Comparison of spine motion in elite golfers with and without low back pain, Journal of Sports Sciences, 20(8). , 599-605, DOI: 10.1080/026404102320183158
23. Martínez, M.L. (2002). Medicina Manual Osteopática. Revista Facultad de Medicina, 50(3)., 162-6.
24. McHardy, A. & Pollard, H. (2005). Golf and upper limb injuries: a summary and review of the literatura. Chiropractic & Oteopathy, 13(7)., doi:10.1186/1746-1340-13-7
25. Perry, A., Wang, X., Feldman, B., Ruth, T. & Signorile, J. (2004). Can laboratory-based tennis profiles predict field test of tennis performance? J Strength & Conditioning Research, 18(1). , 136-143.
26. Robles, A. (2010). Efecto agudo y a largo plazo de la técnica active isolated stretching sobre el rango de movimiento y la fuerza [master's thesis]. Spain: University of Granada.
27. Rodríguez García, P.L. & Moreno Murcia, J.A. (1997). Justificación de la continuidad en el trabajo de estiramiento muscular para la consecución de mejoras en los índices de amplitud articular. Apunts. Educación física y deportes, 2(48)., 54-61.
28. Rojas -Valverde, D., Gutiérrez-Vargas, R., Sánchez-Ureña, B., Gutiérrez Vargas, J.C., Cruz-Fuentes, I. & Salas-Cabrera, J. (2015). Comportamiento neuromuscular posterior a la competencia en jugadores profesionales de fútbol de Costa Rica: un seguimiento tensiomiográfico. Revista Pensar en Movimiento: Ciencias del Ejercicio y la Salud, 13(2).
29. Rojas-Valverde, D., Gutiérrez-Vargas, R., Sánchez-Ureña, B., Gutiérrez Vargas, J.C. & Hernández-Castro, A. (2016). Estat del balanç neuromuscular i massa magra d’extremitats inferiors de jugadors professionals de futbol de la primera divisió de Costa Rica. Revista Apunts: Educación Física y Deporte, 125, 63-70.
30. Rojas-Valverde, D., Gutiérrez-Vargas, R., Rodríguez-Montero, A., Pereira, L., Loturco, I. & Martín-Rodríguez, S. (2018). Reduced muscle contractile function in elite young soccer players after a short-congested fixture period. Journal of Sports Engineering and Technology, (In press).
31. Rubini, E. C., Pereira, M. I., & Gomes, P. S. (2005). Acute effect of static and PNF stretching on hip adductor isometric strength. Med Sci Sports Exerc, 37(5)., S183-184.
32. Sánchez-Ureña, B., Rojas-Valverde, D. & Gutiérrez-Vargas R. (2018). Acute immersion protocol is not effective for neuromuscular mechanical function recovery: a tensiomyography study. Frontiers in Physiology, 9, 766.
33. Shearar, KA, Colloca, CJ, White, HL. (2005). A randomized clinical trial of manual versus mechanical force manipulation in the treatment of sacroiliac joint syndrome. J Manipulative Physiol Ther, 28(7)., 493-501.
34. Snow, R. (2016). Task force on the low back pain clinical practive guidelines. J Am Osteopathic Assoc, 116, 536-549.
35. Suter E, McMorland G, Herzog W, Bray R. (2000). Conservative lower back treatment reduces inhibition in knee-extensor muscles: a randomized controlled trial. J Manipulative Physiol Ther, 23, 76-80.
36. Towlson, C., Midgley, A. W., & Lovell, R. (2013). Warm-up strategies of professional soccer players: practitioners’ perspectives. Journal of Sports Sciences, 31(13)., 1393-401.
37. Triano, J. (2001). The mechanics of spinal manipulation. In: Herzog, W., editor. Clinical biomechanics of spinal manipulation (pp. 92-190). New York: Churchill Livingstone.
38. Vad, V., Bhat, A. & Basrai, D. (2004). Low back pain in professional golfers. The American Journal of Sport Medicine, 32(2)., 494-497.
39. Williams, N. (1997). Managing back pain in general practice--is osteopathy the new paradigm? British Journal of General Practice, 47(423). , 653-655.